Goals
- Learn the importance of initial stay sutures just proximal and distal to the intended gastrojejunal anastomosis.
- Learn gentle handling of tissue edges to be anastomosed.
- Learn the four layers of a side-to-side intestinal anastomosis.
- Learn how to transition from the posterior interlocking (hemostatic) mucosal suture that approximates the stomach to the jejunum to the anterior inverting mucosal suture at the proximal and distal ends of the anastomosis by using a Connell suture technique. This is known as “turning the corner” and is a critical step in avoiding subsequent anastomotic leak.
Equipment
- Goat stomach and at least 60 cm of attached small bowel. Note: The goat’s stomach anatomy is quite different from human gastric anatomy. The goat is a ruminant and has four stomach compartments. The part just proximal to the pylorus—known as the abomasum or true stomach—is the best part to use for this exercise.
- 17 inch x 24 inch plastic cutting board.
- Scalpel with #10 blade.
- Metzenbaum scissors.
- Surgical forceps.
- Needle holder.
- 3-0 silk suture on an atraumatic curved needle.
- 2 curved small hemostats.
- Suture scissors.
Preparation
- Irrigate the goat stomach and the attached small intestine with copious amounts of water to clear of digestive contents.
- Place the goat stomach on the cutting board.
- Select a segment of jejunum to anastomose to the stomach just proximal to the pylorus along the greater gastric curvature.
Lesson
Performing a Gastrojejunostomy
1. Place 3-0 silk stay sutures 1 cm beyond the proximal and distal ends of the planned gastrojejunostomy.

Figure 1: Placement of Stay Sutures
2. Make an incision in the stomach that ends 1 cm from the two stay sutures (see below).
Note: In the human setting the cut edges will bleed. Do not use excessive cautery as this will risk necrosis of the bowel wall. Ligate large bleeders. Oozing bleeders will stop on their own.
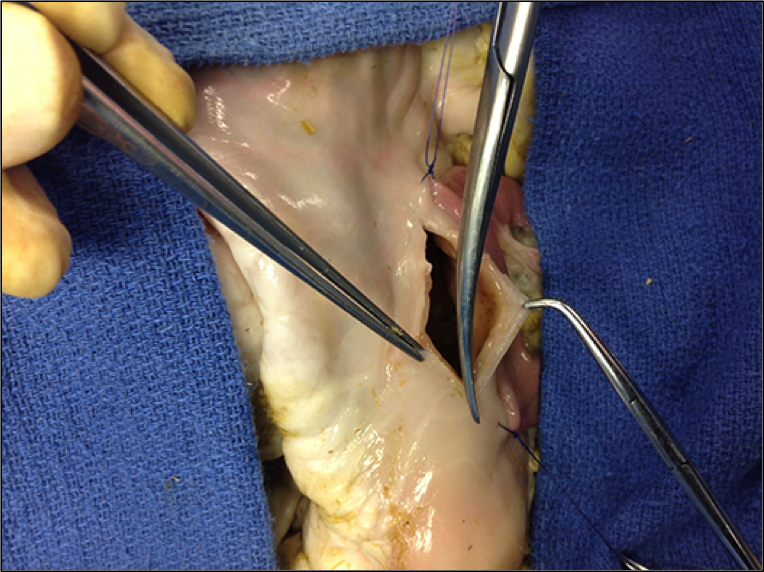
Figure 2: Gastric Incision
3. Make an incision in the jejunum parallel to the gastric incision (see below).
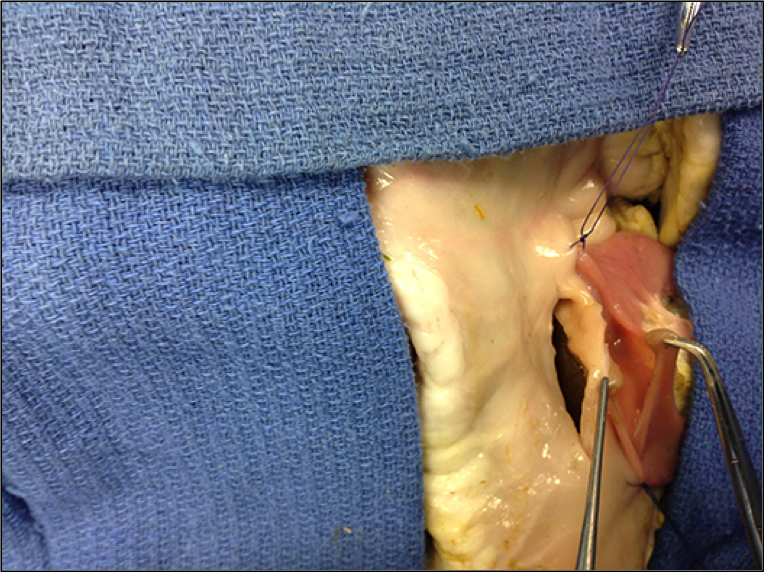
Figure 3: Jejunal Incision
4. Place seromuscular interrupted 3-0 silk sutures on an atraumatic needle between the posterior gastric wall and the adjacent posterior jejunal wall (see below). This is known as the posterior seromuscular layer of the anastomosis.
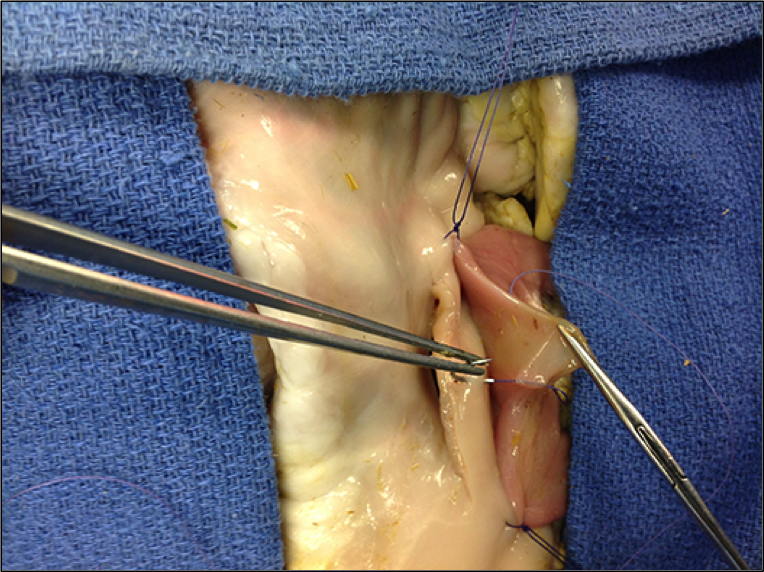
Figure 4: Initial Posterior Seromuscular Suture
5. Place two full-thickness sutures through the adjacent gastric and jejunal walls posteriorly (see below). Then run one suture proximally and one suture distally interlocking the sutures for hemostasis. This is the second posterior anastomotic layer.
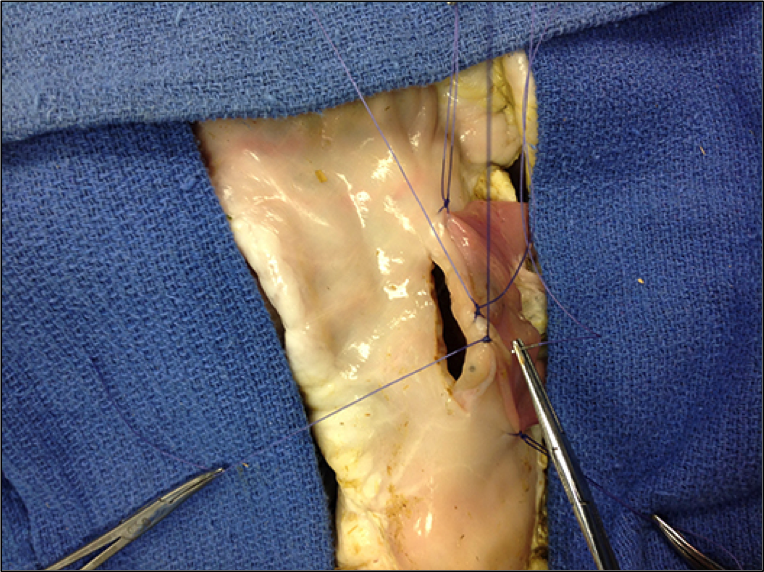
Figure 5: Jejunum Approximated to Stomach with Initial Proximal and Distal Sutures
6. Turning the anastomotic angle using Connell suture technique (see below). Using the distal interlocking posterior anastomotic suture, drive it starting through the mucosa and then full thickness through the distal gastric wall.
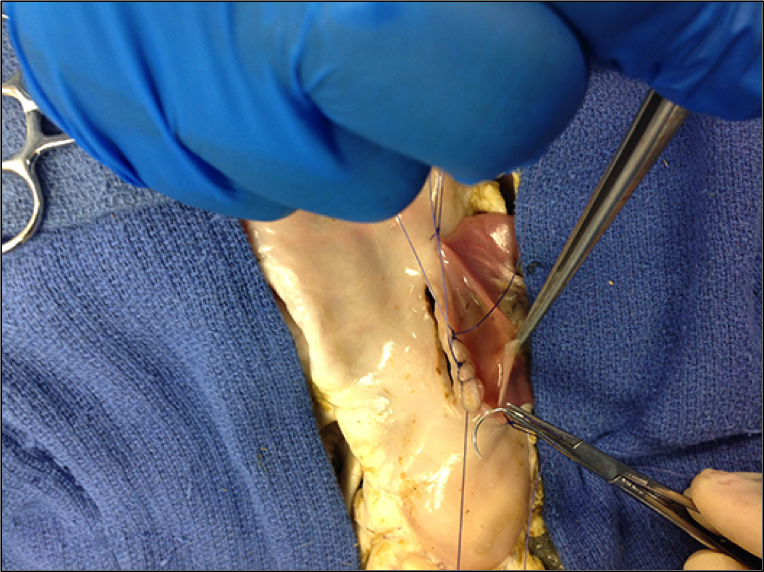
Figure 6: Initial Connell Suture Passing Inside Out Through the Distal Jejunal Wall
7. Then pass the same suture outside in through the full thickness of the adjacent distal gastric wall (see below).
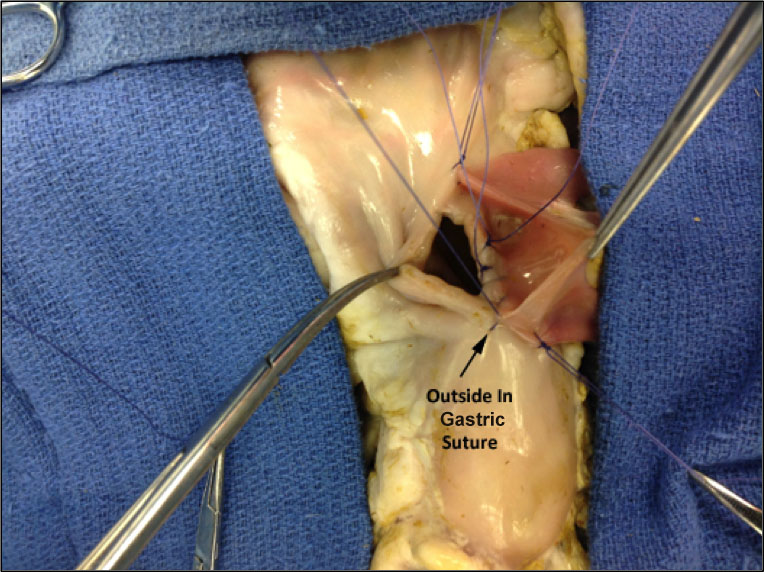
Figure 7: Outside In Gastric Suture
8. Next, turn the suture and pass it full thickness back inside out through the gastric wall (see below).
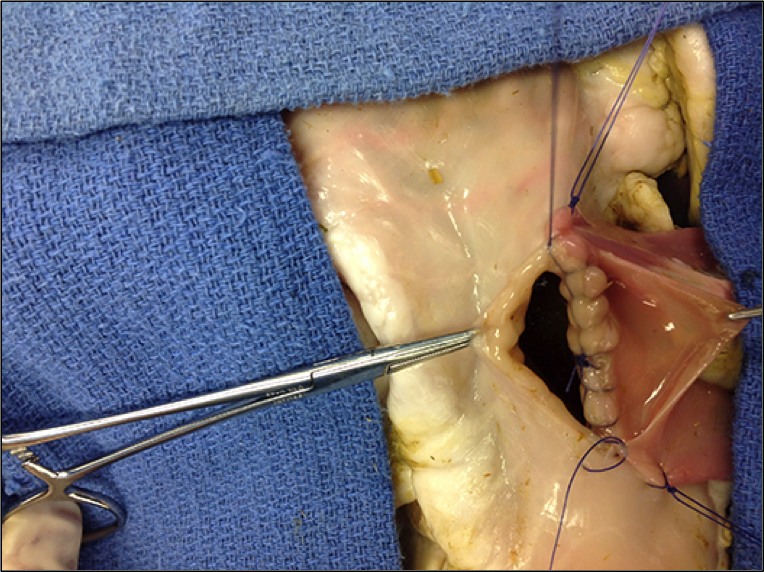
Figure 8: Inside Out Gastric Suture
9. Repeat the same process with the previously placed proximal suture after running it proximally with interlocking sutures to the angle of the anastomosis. Then use the Connell suture technique to turn the proximal anastomotic angle (see below). This maneuver inverts the mucosal layer.
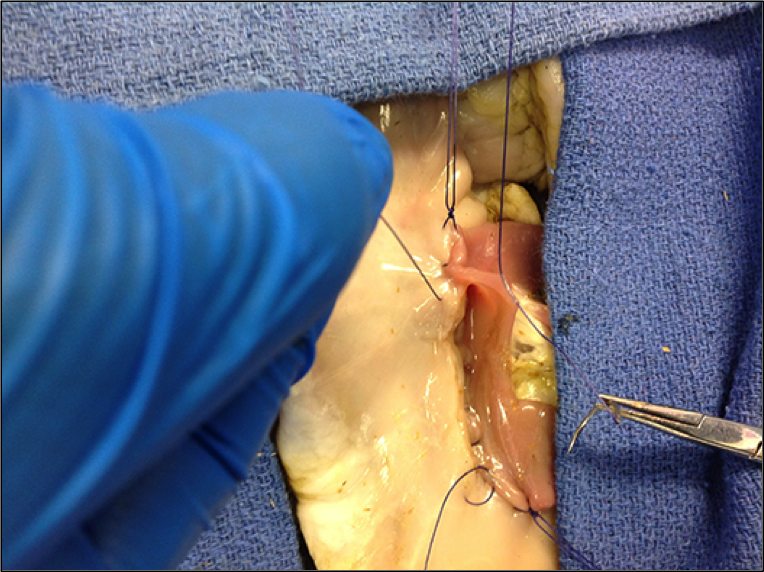
Figure 9: Closing Proximal Angle with Connell Sutures
10. Complete the anterior mucosal inverting layer by placing outside in and then inside out full thickness sutures through the gastric and adjacent jejunal walls (see below).
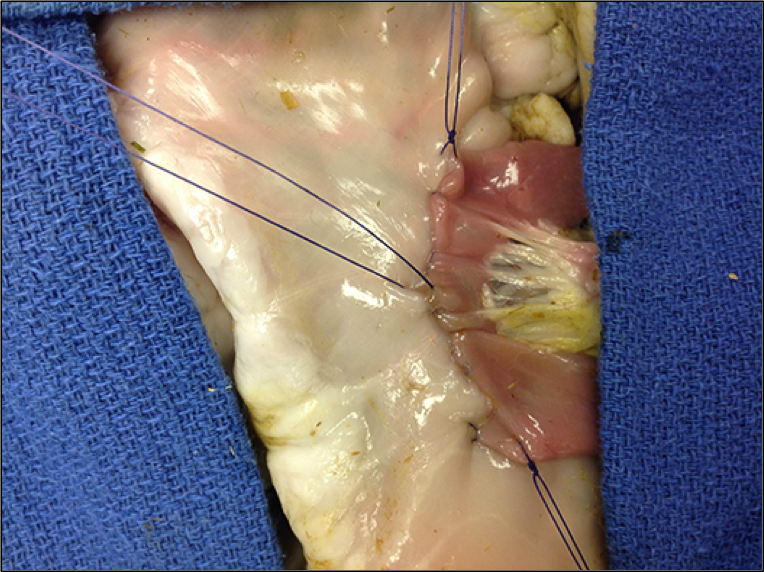
Figure 10: Anterior Inverted Gastrojejunal Anastomosis
11. The final step in the gastrojejunostomy is to place a second layer of interrupted seromuscular sutures anterior to the previously placed inverting mucosal layer.
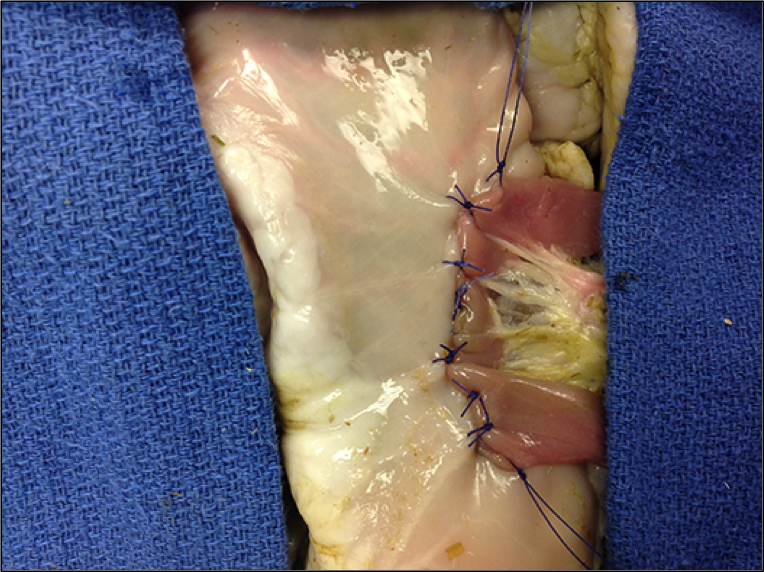
Figure 11: Interrupted Anterior Seromuscular Suture Layer
12. Cut the ends of the stay sutures leaving the knots in place. Place a seromuscular suture just beyond the anastomosis at each end to reinforce the angle.